“It all started as a rumour… Then we found we
were dealing with a disease. Then we realised that it was an epidemic.
And, now we have accepted it as a tragedy.” - Chief epidemiologist in
Kampala, Uganda

A complex computer model of the evolution of HIV-1 has suggested that the first transfer of SIV to humans occurred around 1930, with HIV-2 transferring from monkeys found in Guinea-Bissau, at some point in the 1940s .
Studies of primates in other continents did not find any trace of SIV, leading to the conclusion that HIV originated in Africa.
The 1960s- Early cases of AIDS
Experts studying the spread of the epidemic suggest that about 2,000 people in Africa may have been infected with HIV by the 1960s. Stored blood samples from an American malaria research project carried out in the Congo in 1959 prove one such example of early HIV infection.
The 1970s – The first AIDS epidemic
It was in Kinshasa in the 1970s that the first epidemic of HIV/AIDS is believed to have occurred. The emerging epidemic in the Congolese capital was signalled by a surge in opportunistic infections, such as cryptococcal meningitis, Kaposi’s sarcoma, tuberculosis and specific forms of pneumonia.
It is speculated that HIV was brought to the city by an infected individual who travelled from Cameroon by river down into the Congo. On arrival in Kinshasa, the virus entered a wide urban sexual network and spread quickly. The world’s first heterosexually-spread HIV epidemic had begun.
The 1980s – Spread and reaction
Although HIV was probably carried into Eastern Africa (Uganda, Rwanda, Burundi, Tanzania and Kenya) in the 1970s from its western equatorial origin, it did not reach epidemic levels in the region until the early 1980s .
Once HIV was established rapid transmission rates in the eastern region made the epidemic far more devastating than in West Africa, particularly in areas bordering Lake Victoria. The accelerated spread in the region was due to a combination of widespread labour migration, high ratio of men in the urban populations, low status of women, lack of circumcision, and prevalence of sexually transmitted diseases 9. It is thought that sex workers played a large part in the accelerated transmission rate in East Africa; in Nairobi for example, 85 percent of sex workers were infected with HIV by 1986 .
Uganda was hit very hard by the AIDS epidemic in the 1980s. At the beginning of the decade, doctors were confronted by a surge in cases of a severe wasting disease known locally as ‘slim disease’, alongside a large number of fatal opportunistic infections such as Kaposi’s sarcoma. By this time doctors were aware of AIDS cases with similar symptoms in the United States:
‘But we just could not connect a disease in white, homosexual males in San Francisco to the thing that we were staring at…’ David Serwadda, former medical resident at the Uganda Cancer Institute in Kampala.
After the initial clinical recognition of the link between ‘slim disease’ and AIDS, research was initiated to discover transmission patterns, risk factors, and the prevalence of HIV in Uganda. By the end of the decade HIV prevalence amongst pregnant women in Uganda’s capital had peaked at over 30 percent.
Confusion, stigma and despondence

West Africa had generally high levels of infection of both HIV-1 and HIV-2, although nowhere near the proportions of East Africa. The HIV-1 epidemic spread across the region beginning with reported cases in Côte d’Ivoire (probably due to rapid urbanisation and immigration) . By the end of the decade HIV infection had been identified in all of the West African states. Sex work was also a major driver of early infection in West Africa; in Abidjan the former capital of Côte d’Ivoire, the HIV prevalence amongst sex workers was already 38% by 1986.
In the mid-1980s the Western African nation of Guinea-Bissau had the world’s highest level of HIV-2, with 26% of paid blood donors, 8.6% of pregnant women and 36.7% of sex workers testing positive . The virus spread into rural areas of southern Senegal and the Gambia but HIV-2 was not infectious enough to generate an epidemic beyond this region.
Truck drivers – alongside other migrants such as soldiers, traders and miners – have been identified as a group which facilitated the initial rapid spread of HIV-1, as they engaged with sex workers and spread HIV outwards on the transport and trade routes. In the 1980s, 35 percent of tested Ugandan truck drivers were HIV positive, as were 30 percent of military personnel from General Amin’s Ugandan army.
In 1988 the second highest prevalence rate of HIV in all of Africa was found on the Tanzam road linking Tanzania and Zambia .
As the decade progressed so too did the epidemic, moving south through Malawi, Zambia, Mozambique, Zimbabwe and Botswana.
Although the virus arrived comparatively late in this region it spurred a devastating epidemic in the general population. By the end of the 1980s the southern African countries of Malawi, Zambia, Zimbabwe and Botswana were on the verge of overtaking East Africa as the focus of the global HIV epidemic.
It is thought that the first case of HIV in South Africa was in a white, homosexual air steward from the USA who died of pneumonia (PCP) in 1982. Blood specimens showed a 16 percent infection rate among tested gay men in Johannesburg in 1983. The small-scale epidemic was largely confined to white gay men and remained virtually unheard of in the general population in the mid 1980s. The homosexual epidemic had stopped growing by the end of the decade.
Confusion, stigma and despondency
The 1980s in Uganda was characterised as a period of patashika (confusion) and rumour abounded as to the nature of AIDS. The cause of AIDS was still unclear in the early eighties although it was ‘thought to be an infectious agent, probably a virus’ . Very little was known about transmission and public anxiety was high. ‘They are all simply bewildered’ said a Ugandan health worker.
Many questions remained unanswered, most significantly what causes AIDS and how it is transmitted. There were numerous misconceptions, with people thinking that ‘you can get HIV through an apple or an orange or an injection or anything’ or ‘a fat person didn’t have HIV’ or ‘HIV can be transmitted just by looking at a person’ . Additionally, confusion with other diseases such as malaria led to over-estimations of the transmissibility of HIV and added to the fear surrounding the virus.
Fear quickly bred stigma towards those infected with HIV. Stigma was often related to the association of HIV with prostitution, promiscuity and high-risk lifestyles.
“In the early days, when it first came, it was a disease for prostitutes. There were posters with a guy and a bottle of beer and a lady in a miniskirt. Those were the ones that were supposed to get HIV”Because not much was known about HIV/AIDS in the mid-1980s people were often not aware that they were infected with HIV until they had progressed to the final stages of the disease when death was often imminent. This fact coupled with the lack of any effective preventative therapies or treatment, meant that there was a reluctance to be tested for the virus.
“Why get tested if there was no treatment and no cure – if you were sent home to die, shunned by your family and neighbours”.
Government responses to AIDS
With a few notable exceptions, the 1980s were characterised by an insufficient response to AIDS in Africa. Often government capacity was saturated by immediate economic concerns, war or political crisis.
As there was no treatment or cure for HIV infection or AIDS in the 1980s, government strategies had to focus on prevention. Prevention efforts often include encouraging people to revise their sexual behaviour, by abstaining from sex or delaying first sex, being faithful to one partner or having fewer partners, or using condoms consistently and correctly. For this reason prevention efforts in Africa were often confronted with opposition from religious authorities. Both Muslim and Christian leaders found prevention campaigns such as condom promotion difficult to reconcile with their teachings, despite prevailing evidence that abstinence and mutual monogamy were perhaps not as common as they would like.
UNAIDS reported that;Many senior politicians were reluctant to admit to a generalised HIV/AIDS epidemic in their country for fear of creating panic, or discouraging tourism . For this reason it was significant that in 1987 President Kenneth Kaunda of Zambia, a respected African leader, announced to the world that his son, Masuzyo, had died of AIDS.
“The fear of offending powerful religious constituencies… created gridlock in some national governments, and for good reason. Conservative lobbies have shown that they can obstruct everything from family life and education to condom promotion if they chose” .
Uganda and Senegal are often cited as countries that did respond quickly and effectively to the AIDS crisis.
Senegal has one of the lowest rates of HIV in sub-Saharan Africa. The international community often attribute this low prevalence to the prompt response of the government and community organisations to the epidemic, although UNAIDS concedes that it is impossible to predict how the epidemic would have progressed without intervention.
It was not until 1986 when the Ugandan civil war ended and President Museveni was firmly in power that the country got behind a prevention programme. By this time the country was in the midst of a major epidemic, with a prevalence rate of 26% in its capital city.
In 1987 Uganda’s AIDS control programme formulated a five-year plan with the assistance of the World Health Organisation (WHO). The plan was later made a model for Africa and received more than £20 million in donor funding. The main principles of the campaign were openness and frankness.
Other African nations did not respond to the HIV/AIDS epidemic so positively. In fact, President Mobutu of the Congo banned the subject from the press for four years between 1983 and 1987 and Zimbabwean doctors were instructed not to mention AIDS on death certificates.
South Africa’s white leaders refused to install an AIDS education programme in schools and did not begin to take seriously the danger of a large-scale heterosexual HIV/AIDS epidemic until the end of the decade.
Global response to AIDS in Africa The World Health Organisation was slow to respond to the emerging HIV/AIDS epidemic in Africa as it contended that AIDS was not the primary healthcare concern in the region. In 1985 Halfdan Mahler, the Director-General of the organisation said ‘AIDS is not spreading like bush fire in Africa. It is malaria and other tropical diseases that are killing millions of children every day’ . Realising quickly the inaccuracy of this statement, the following year Mahler admitted that ‘[e]verything is getting worse and worse in AIDS and all of us have been underestimating it, and I in particular’. The WHO Global Programme for the Fight against AIDS was swiftly put into action and aimed to raise $1.5 billion a year by the end of the decade to help prevention and educational efforts , with priority to Africa .
In 1987, Jonathon Mann, the director of the Global Programme estimated that one to several million Africans may already have been infected with HIV.
The 1990s – Southern Africa and the fight for treatment
The beginning half of the 1990s was a bleak time in the history of AIDS in Africa. At a time when new HIV infection rates were rocketing in Southern Africa there were few new ideas of how to deal with generalised epidemics in poor countries.

“AIDS is not just a serious threat to our social and economic development, it is a real threat to our very existence, and every effort must be made to bring the problem under control.”
Although HIV/AIDS prevalence continued to increase in Southern Africa in the later Nineties, glimmers of hope for the future of the epidemic began to emerge.
HIV prevalence in many East African countries that were hard hit in the 1980s was beginning to slow, stabilise or decline. Between 1992 and 1998 adult HIV prevalence in Uganda was estimated to have dropped from 30% to 12% in Kampala .
In 1996, UNAIDS was established to take responsibility for coordinating international action against the epidemic.
Rocketing prevalence in sub-Saharan Africa
Sub Saharan Africa was the hub of the HIV epidemic of the 1990s. In 1993 there were an estimated 9 million people infected in the sub-Saharan region out of a global total of 14 million.
In 1998 sub-Saharan Africa was home to 70% of people who became infected with HIV during the year, with an estimated one in seven of these new infections occurring in South Africa.
As HIV/AIDS entered the southern African countries with force, those infected faced high levels of stigma. In 1998, Gugu Dlamini, a South African AIDS activist, was beaten to death by her neighbours after revealing her HIV positive status on Zulu television. This happened just a month after Deputy President Thabo Mbeki had called for people to ‘break the silence about AIDS’ in order to defeat the epidemic.
South Africa had reacted slowly to the emerging epidemic. The ANC had replaced the apartheid government in 1994 and had concentrated on unifying the country’s health systems and expanding primary health care for the poor. This restructuring weakened the health systems just as the HIV/AIDS epidemic was at the peak of expansion. In 1998 the health ministry stopped trials of AZT to prevent mother-to-child-transmission claiming that it was too expensive and that it would focus its funds on other prevention campaigns. This provoked the first major political action by HIV positive Africans over their own treatment.
The ANC did not work with AIDS organisations and tension between the party and AIDS activists escalated throughout the decade. Due to an increasing frustration with the governments inefficient action against AIDS, in 1998 the Treatment Action Campaign (TAC) was founded. Led by Zackie Achmat, this group was to become important in the fight for treatment in South Africa.
The Fight for Treatment
In 1996 the effective combination therapy known as HAART became available for those living with HIV in rich countries. The new drugs were so effective that AIDS death rates in developed countries dropped by 84% over the next four years . This led scientists to declare, “aggressive treatment with multiple drugs can convert deadly AIDS into a chronic, manageable disorder like diabetes”.
However, as the South African Health Minister, Nkosazana Zuma, pointed out,
“most people infected with HIV live in Africa, where therapies involving combinations of expensive antiviral drugs are out of the question”.
At a cost of $10,000-15,000 per person per year it would have cost sub-Saharan countries between 9% and 67% of their GDP to provide triple combination therapy to everybody living with HIV in their countries.
This was impossible for the majority of African nations and the disparity in treatment options angered many people for whom treatment was too expensive. South Africa began to lobby the multi-billion-dollar pharmaceutical corporations of the West to either allow local companies to manufacture HIV/AIDS drugs themselves (compulsory licensing) or import them from other countries, that were producing generic (or copied) drugs at a low cost (parallel importing).
The drug companies argued that if their patents were not protected, there would not be the incentive to do the research and development necessary to continue the fight against AIDS60 , and they fought vigorously to protect their privileges. The US sided with the pharmaceutical companies and threatened tough sanctions against South Africa .
Eventually, in December 1999 the US and the pharmaceutical companies backed down and Bill Clinton announced that the United States would exercise flexibility in the enforcement of drug patent laws when countries face a public health crisis . The United States approved local production or importation of cheap HIV drugs in South Africa as long as the imported drugs had intellectual property right protection.
This was an initial victory for the fight for treatment in resource poor countries but did not signal an immediate roll out of drugs for those living with AIDS in Africa. For a start not every country had the industry to manufacture drugs locally, or the money to import the drugs, even at a lower cost.
Additionally, this treatment was demanding of clinical services and many governments did not have the healthcare infrastructure to manage large-scale treatment programmes. In the 1980-1990s, sub-Saharan Africa had the world’s lowest level of social security cover, which includes doctor/patient ratio and access to health services.
Another medical advance was the discovery, in 1994, that the antiretroviral drug zidovudine (AZT) could reduce mother-to-child transmission by two-thirds. Although this transformed transmission through pregnancy in developed countries, the cost of about $1,000 per case was prohibitive in poorer countries. After trials in Thailand showed that a shorter course of AZT also helped to prevent mother-to-child transmission of HIV , the drug company Glaxo Wellcome cut the price of AZT by 75% in 1998. Peter Piot, director of UNAIDS, praised the ‘hope factor’ of the drug and in 1999 Botswana launched Africa’s first programme to combat mother-to-child transmission.
The 2000s – Global initiatives and drugs roll out

“In this effort, there is no us and them, no developed and developing countries, no rich and poor – only a common enemy that knows no frontiers and threatens all people.” Kofi Annan at the G8 summit in Genoa
In 2000, after mounting pressure to make AIDS drugs more accessible, five pharmaceutical companies offered to negotiate steep reductions in the prices of AIDS drugs for Africa and other poor regions . The production of generic drugs by local pharmaceutical in countries like India and Brazil had sparked a ‘price war’ between the pharmaceutical giants like GlaxoSmithKline and generic drug makers.
The negotiations were lengthy but over the following few years the world’s biggest drug manufacturers frequently cut the price of various patented AIDS drugs until they were only marginally more expensive than the recently approved generic (or ‘copied’) drugs
The production of generic drugs and resulting price reductions were only the first step on the ladder towards universal access to AIDS treatment. Peter Piot, the executive director of UNAIDS said:
“This is a promising step in a long-term process… Lowering the price of medicines, however, is only one critical factor in what must become a broader and more urge nt effort”Practical issues were also of concern as there was widespread scepticism regarding the feasibility of rolling out antiretroviral treatment to those living with HIV in Africa. The concerns centred on the weak healthcare infrastructure (in 2005 there was a shortage of 1 million professional health workers in Africa) or patients’ inability to adhere to treatment (as not taking the drugs at the correct time can lead to drug resistance). This particular concern was proven to be unfounded; in fact HIV positive patients in sub-Saharan Africa have been found to have higher rates of adherence to HIV treatment than those in America. The physical delivery of the drugs to remote parts of Africa was also a concern.
In 2001 there were more than 20 million people (based on current estimates) living with AIDS in sub-Saharan Africa, but only 8,000 people were accessing drug treatment.
Joep Lange, the President of the International AIDS Society was optimistic:Although the ‘3 by 5’ target was not met, the campaign did manage to substantially increase the number of people on treatment in Africa and raise political support and financial commitment for HIV/AIDS in resource poor countries.
“If we can get cold Coca Cola and beer to every remote corner of Africa, it should not be impossible to do the same with drugs”.
The debate about the feasibility of providing AIDS drugs to Africa was effectively silenced by the so-called ‘3 by 5’ initiative unveiled by the WHO in 2003. The ambitious programme aimed to put 3 million people in developing countries on antiretrovirals by the end of 2005.
Between 2003 and 2005 the number of people receiving treatment for HIV/AIDS in sub-Saharan Africa increased more than eight-fold from 100 000 to 810 000 people .
At last it seemed that the world was sitting up and taking notice of the ravaging AIDS epidemic in Africa. The amount of money that Western nations were willing to give to help scale-up treatment for those living with AIDS in Africa increased in the new millennium. In 2001, The Global Fund to Fight AIDS, Tuberculosis and Malaria was created79 80 81 and two years later United States President George Bush announced the President’s Emergency Plan For AIDS Relief (PEPFAR) .
Overall between 2001 and 2004 global funding for AIDS in low- and middle-income countries (from national, private and international sources) more than trebled from $1.8 billion83 to $6.1 billion.
Roll Out

Addressing the UN assembly in June 2001, President Festus Mogae of Botswana voiced his fears of the impact that HIV/AIDS was having on his country.
“We are threatened with extinction. People are dying in chillingly high numbers. It is a crisis of the first magnitude.”The following year Botswana became the first African country to launch a national antiretroviral treatment project. MASA (meaning ‘new dawn’) was to be equally financed by the Botswana government, the Gates Foundation and the drugs company Merck. Treatment uptake was slow at first as there was a major shortage of health workers and even these few cases overwhelmed the health system. The programme gained momentum and by 2007 approximately 95% of HIV positive people in the country were being treated.
Botswana’s successful treatment programme allayed doubts that antiretroviral treatment for poor African countries was unfeasible. Its programme has been by far the most successful in Africa, although Namibia (treating 71% of those in need in 2006), Rwanda (72%), Kenya (44%), Malawi (43%) Swaziland (42%) Uganda (41%), have also been regarded as reasonably successful at rolling out treatment.
Less successful have been Sudan and Somalia (civil conflict means that data is extremely difficult to collect, estimates lie at around 1% coverage), and Nigeria (due to its extremely weak health system, only 15% of people in need were receiving treatment by 2005).
UNAIDS reported that in total around 17% of those in need of the life-saving drugs in sub-Saharan Africa were receiving them in 200588 . This had increased to 42% by 2008.
Although access to treatment in sub-Saharan Africa greatly expanded in the first decade of the 21st century, a change in WHO guidelines in 2010 led to an increased number of people estimated to be in need of treatment. The new guidelines which recommend starting treatment at an earlier stage (when a patient’s CD4 count that has dropped below 350 cells/mm3 of blood as opposed to 200 cells/mm3), mean that treatment coverage in sub-Saharan Africa in 2009 was 37%. According to the previous WHO guidelines (2006), treatment coverage would have reached 53% in 2009.
South Africa’s national HIV treatment programme has been the topic of much debate. The South African government was initially hesitant about providing antiretroviral treatment to HIV positive people, due to unconventional views about HIV and AIDS within the government, including President Mbeki’s questioning of whether HIV really causes AIDS. After pressure from activists, specifically the Treatment Action Campaign (TAC) the state began to supply ARV drugs in 2004. But even since treatment began the distribution of antiretroviral drugs was relatively slow, with only around 37% of people in need receiving treatment at the end of 2009 according to the latest WHO guidelines. The year 2010 marked an important year in the history of AIDS in South Africa as an ambitious national HIV counselling and testing campaign was rolled out and task-shifting (delegating some doctors’ tasks to nurses and community workers to reduce the burden on health systems) was implemented. However, the difficulties that South Africa will face in turning back the tide on its AIDS epidemic were made clear by the lower than expected number of tests carried out in the first months of the campaign, prolonged public sector strikes involving health workers, and ARV drug stockouts.
In a decade in which ethical issues were rising up the corporate agenda, a number of large companies also began to provide AIDS treatment programmes for their employees. The vice-president of Anglo American, a large South African mining firm explained that the cost for the firm was justified as the dramatically reduced absenteeism compensated for three-quarters of the cost of the treatment programme.
Prevalence and behaviour change
UNAIDS reported in 2006 that there had been a behavioural change in some parts of Africa in the new millennium. This was believed to be partly due to increased condom use since the early 1990s, as well as young people delaying first sex and reducing the number of casual sex partners . This trend may have accounted for the reported decline in HIV prevalence in some parts of Africa, notably Kenya, Zimbabwe and urban areas of Burkina Faso. However, the decline was also likely to be a result of high-mortality rates. In 2010, it was revealed that HIV infections had reduced by more than a quarter between 2001 and 2009 in 22 countries in Africa, including among young people and women.
Elsewhere in southern Africa HIV prevalence levels appeared to have levelled off by 2006 (i.e. the number of new infections roughly matched the number of people dying of AIDS) although the stabilization was at very high levels. This trend continued as the end of the first decade came to a close.
In 2009 1.3 million people in sub-Saharan Africa died of AIDS.
It was estimated in 2007 that since the beginning of the epidemic more than 15 million Africans had died from AIDS , equivalent to the combined populations of London and New York. In this context it becomes possible to understand the massive impact that the AIDS epidemic has had on families, communities, workplaces and national and regional development in Africa.
Rapid increases in bilateral donations (especially from the U.S) and the creation of funding mechanisms like the Global Fund led to a record increase in funding for the AIDS epidemic, from $1.8 billion in 2001 to $15.6 billion in 2008 . However, the financial crisis (2007-present) started to have a noticeable effect on the provision of funding. In 2009, global funding remained flat; a marked change from the substantial increase. In 2010, Uganda reported that they had to end new enrollment on antiretroviral treatment programmes because of a cap on PEPFAR funds. Although PEPFAR later lifted the cap following substantial media coverage and promised renewed funds, the effect of the ‘donor retreat’ from HIV and AIDS funding had already become clear. In 2009, UNAIDS and the World Bank released a report regarding the impact of the financial recession on the epidemic. A report in 2010 also noted how funding commitments were having an impact on work on the ground in eight countries in Africa, stalling the scale up of treatment, prevention and care services and increasing the frequency of drug stock outs .
The history of AIDS in Africa is far from complete. Not only will the effects of the current epidemic be felt for generations to come, but the lack of a cure for AIDS coupled with limited access to treatment in Africa means that the worst is still not over and millions of people will continue to suffer the multiple impacts of the AIDS epidemic.
“When this whole thing is over, everyone will stop and cry. But at this point we are numb.” Winstone Zulu, Zambian AIDS activist
HIV / AIDS pandemic affects development in Africa
developAfrica
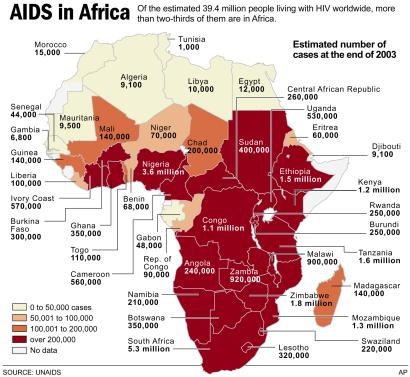
Africa disproportionately bears the burden of the HIV/AIDS pandemic. Although only 11% of the world's population lives in Africa, roughly 67% of those living with HIV/AIDS are in Africa. In Africa, there were 22.4 million people living with HIV and 1.9 million new HIV infections in 2008. An estimated 14 million children in Africa have been orphaned as a result of HIV/AIDS.
See
1. WHO. Facts about health in the African Region of WHO. Available at: http://www.who.int/mediacentre/factsheets/fs314/en/index.html
2. UNAIDS. Global facts and figures: The global AIDS epidemic. Available at: http://data.unaids.org/pub/FactSheet/2009/20091123_FS_global_en.pdf
developAfrica
Africa disproportionately bears the burden of the HIV/AIDS pandemic. Although only 11% of the world's population lives in Africa, roughly 67% of those living with HIV/AIDS are in Africa. In Africa, there were 22.4 million people living with HIV and 1.9 million new HIV infections in 2008. An estimated 14 million children in Africa have been orphaned as a result of HIV/AIDS.
See
1. WHO. Facts about health in the African Region of WHO. Available at: http://www.who.int/mediacentre/factsheets/fs314/en/index.html
2. UNAIDS. Global facts and figures: The global AIDS epidemic. Available at: http://data.unaids.org/pub/FactSheet/2009/20091123_FS_global_en.pdf
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου